Spinal Surgery
Disorder of the Spinal Column
Spine surgery includes treatment of the spinal column, or the support structures around the spinal cord and spinal nerves. Compression or constriction of the nerves and spinal cord by the bony overgrowth of the spine or herniated disks can cause pain, sensory changes or weakness. Treatment often requires decompression (removal of abnormal bone growth/herniated disks) of the spinal cord and nerves to alleviate symptoms. Spinal column disorders requiring surgery range from degenerative processes to traumatic injury to tumors. In some circumstances, the stability of the spine is affected. When needed, spinal fusion with or without instrumentation or “hardware” is used to re-establish spinal stability. Minimally invasive techniques and microsurgical techniques are utilized when appropriate to get the best results for the patient.

Regions of the Spine
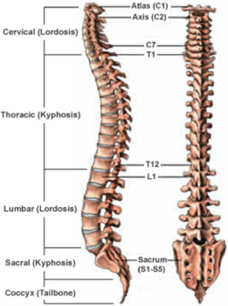
Humans are born with 33 separate vertebrae. By adulthood, we typically have 24 due to the fusion of the vertebrae in the sacrum.
- The top 7 vertebrae that form the neck are called the cervical spine and are labeled C1-C7. The seven vertebrae of the cervical spine are responsible for the normal function and mobility of the neck. They also protect the spinal cord, nerves, and arteries that extend from the brain to the rest of the body.
- The upper back, or thoracic spine, has 12 vertebrae, labeled T1-T12.
- The lower back, or lumbar spine, has 5 vertebrae, labeled L1-L5.
- The lumbar spine bears the most weight relative to other regions of the spine, which makes it a common source of back pain.
- The sacrum (S1) and coccyx (tailbone) are made up of 9 vertebrae that are fused together to form a solid, bony unit.
Disorder of the Spinal Cord
Spinal cord disorders that require surgery include tumors or structural abnormalities of the spinal cord. Spinal cord tumors range from benign to aggressive and surgery or biopsy might be needed to obtain a diagnosis and aid in treatment. Some tumors can be completely treated with surgery alone, others might require other therapies in conjunction with surgery. Structural abnormalities of the spinal cord can include dilated, fluid-filled channels in the spinal cord (syrinx, syringomyelia), tethered spinal cords and other developmental problems. Although most of these present in childhood, some become problems as we get older. Surgery in these circumstances helps to alleviate symptoms by altering the structure of the spinal cord.
Disorder of the Spinal Nerve
The problems involving the spinal nerves often come from compression. Degeneration and herniation of the disks in the neck, back and low back can compress spinal nerves as they exit the spinal column. Symptoms can range from numbness to pain to weakness in an arm or leg and difficulty walking. Surgery might include removal of all or part of the disk. If the whole disk is removed, spinal fusion is usually required to maintain the stability of the spine. Degeneration of joints in the spine can also cause spinal nerve compression giving very similar symptoms. Finally, tumors of the nerves themselves can cause pain and dysfunction. All of these can be treated surgically if indicated.
Tumors of the Spine and Spinal Cord
Less common than disorders of the structural elements of the spine, spinal tumors and tumors of the spinal cord also treated by neurosurgeons. These tumors can be metastatic from other parts of the body or can spread from tumors near the spine. These are often cancers and will require other forms of treatment along with or instead of surgery. The tumors of the spinal cord and the nerve roots themselves are often benign and can be treated with surgery alone. We use microsurgical techniques and contact lasers and electrophysiologic monitoring of the spinal cord to improve resection and increase safety.
Surgical Procedures
Most of the surgical procedures for the spine are for decompression of the spinal nerves or spinal cord. The compression can cause pain, weakness and sensory changes that can be reversible with decompression. Surgery is not always the first choice for treatment, but it may be necessary for certain circumstances. Minimally invasive approaches are used, when possible to minimize postoperative discomfort and hasten recovery. The acronym MIS indicates Minimally Invasive Surgery. Listed below are some of the more common procedures performed. This is not a comprehensive list but describes the most common operations done.
Using a tubular retractor system through a 2cm (less than 1 inch) incision we are able to remove a herniated disk and decompress nerve roots. Using an operating microscope and microsurgical instruments increases visualization and decreases the “footprint” of the operation. Intra-operative imaging increases the accuracy of the surgery. The surgery takes about 45 minutes and most patients go home the same day. This one of the most common spinal surgeries performed.
Often decompression of the nerve roots is coupled with a stabilization procedure. This is not a fusion. This procedure allows for decompression of the nerve roots and stabilization of the spine without a bony fusion. Spinal stabilization is done in cases of misalignment of the vertebrae without instability. A decompression might result in instability. After the decompression is done a stabilization device is applied to the spinal segment to prevent instability and preserve motion of the spine. The device used at National Capital Neurosurgery is the coflex. This is often done as an outpatient procedure.
- Lumbar Fusion (Open and MIS)
In cases of instability of the spine associated with spondylolisthesis, a lumbar fusion with decompression is needed. This can be done using an MIS technique using percutaneous pedicle screws or cortical bone screws in an open technique. Fusion is used in cases of instability or fracture. This operation decompresses the spine and fuses the segment(s) that are unstable.
When cervical disks degenerate this can result in nerve root or spinal cord compression. When surgery is needed this often requires complete discectomy and fusion. This is done from an incision in the front of the neck. Microsurgical techniques use sophisticated neurophysiologic monitoring to increase the safety of the surgery. Cervical fusion is often done as an outpatient procedure.
When cervical disk herniations present with otherwise normal anatomy and no significant degeneration of the joints, an artificial disk can be used instead of fusion. Unlike a cervical fusion, the arthroplasty maintains normal motion. It is done using the same microsurgical technique as a fusion, but an artificial disk is used instead of a fusion device. This, too, is almost always an outpatient procedure.
Often abnormal curvature of the spine can lead to pain and neurologic compromise. This can be due to congenital issues, degeneration or from previous surgery. In some circumstances, this “deformity” needs to be corrected. This requires expertise and judgment. Sometimes minimally invasive techniques can be used to achieve the result with short hospital stays and less postoperative discomfort.